C*I*S*H*
Traditionally, a woman with an indication for a hysterectomy has had three choices:
- Subtotal/total abdominal hysterectomy with/without one or both adnexa
- Vaginal hysterectomy with/without one or both adnexa
- Laparoscopy-assisted vaginal hysterectomy with/without one or both adnexa
- Abdominal Hysterectomy (TAH)
- The abdomino/pelvic cavity is entered through a midline or low transverse (Pfannenstiel) incision. Adnexal structures are clamped, divided, and secured with sutures. The bladder reflection is dissected, main vessels are skeletonized, clamped, divided, and secured with sutures. Uterosacral and cardinal ligaments are severed and suture-ligated. The vagina is opened and the uterus removed. Reconstruction of the pelvic floor follows to assure hemostasis and pelvic support.
About 2/3 of all hysterectomies are performed in this manner.
In subtotal hysterectomy the uterine fundus is amputated after ligation of the uterine arteries, leaving the pelvic floor structures intact.
- Vaginal Hysterectomy (TVH)
- This procedure is the "reverse" of the abdominal approach, eliminating the abdominal incision and removing the uterus with/without adnexa vaginally.
About 1/3 of all hysterectomies are performed in this manner.
- Laparoscopy-assisted Vaginal Hysterectomy (LAVH)
- The advent of laparoscopy combines the two previous methods: the abdominal portion is performed laparoscopically, eliminating the abdominal incision. The uterus with/without adnexa is prepared to the extent that it can be removed vaginally.
Depending upon the level of the surgeon's expertise, stages of LAVH have been proposed:
- only the adnexa are severed
- the dissection is carried to but not including the main uterine vessels
- the uterine arteries are divided
- the dissection includes all pelvic floor attachments, the vagina is opened, the uterus removed vaginally, and the pelvic floor reconstructed.
Different names have been attached to these various procedures.
LAVH has converted many otherwise unavoidable abdominal hysterectomies to the more preferable vaginal approach.
All three methods have one thing in common: the surgical breakdown of the pelvic floor! There is interference with the blood and nerve supply to all pelvic organs, support structures are severed, and the vagina is opened. Morbidity is increased. The removal of the cervix is performed in the name of prophylaxis against cervical cancer.
Stimulated and encouraged by the work of RIES, RAURAMO, ALDRIDGE and MEREDITH, and H.REICH, K.SEMM since 1990 has proposed and introduced a different and totally laparoscopic approach to hysterectomy:
C*I*S*H*(Classic Intrafascial S.E.M.M. Hysterectomy)
- C*I*S*H* is a minimal-access, minimally invasive procedure (pelviscopy).
-
C*I*S*H* follows classic surgical techniques, employing only reusable atraumatic forceps, scissors, sutures, and ligatures or thermal endocoagulation for hemostasis.
-
Only diseased structures are repaired or removed. The pelvic floor is kept entirely intact. Blood and nerve supply is left untouched as only the ascending branches of the uterine arteries are ligated. Support structures are not severed and the vagina is not opened. A large tissue cylinder is cored out of the cervix and fundus, removing the functional endocervical mucosa and a large portion of the endometrium. Chronic cervicitis, erosions, eversions are eliminated. The squamocolumnar junction is totally removed, reducing the incidence of stump cancer from about 2% to 0.02%( an incidence of 1:5,000,000).
-
C*I*S*H* can be performed as quickly as any of the other traditional procedures in skilled hands and with a good surgical team.
-
Blood loss and trauma is minimal: only four severed pedicles, a small serosal defect, and the cervical remnant have to heal. Tissue is removed through a suprapubic trocar site with the S.E.M.M.-MotoDrive without having to resort to a colpotomy or extend an abdominal incision.
-
Pain is minimal, recovery fast.
-
C*I*S*H* has the lowest cost: only non-disposable instruments are used. Expensive devices such as lasers, Harmonic scalpel, clips and staples are avoided.
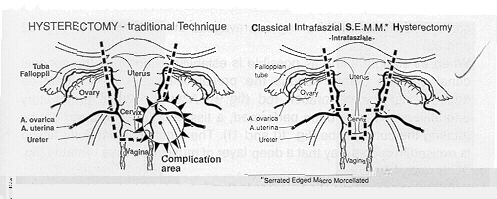
Fig.1 and 2 illustrate the traditional vs. intrafascial hysterectomy. Emphysis is placed on organ preservation, atraumatic approach, and safety for large vessels, ureters, bladder and bowel, keeping morbidity to a minimum.
C*I*S*H* is not an entirely new concept. It is the synthesis of three well established and widely used procedures:
- Supracervical amputation of the corpus uteri
- Conization of the cervix
- Laparoscopy (pelviscopy)
According to HEGEL(1770-1831) THESIS leads to ANTITHESIS, leads to SYNTHESIS
Applied to hysterectomy we remember that subtotal hysterectomy was the standard for fifty years (THESIS). In the last fifty years a switch was made to total hysterectomy (ANTITHESIS). Out of both concepts C*I*S*H* was developed (SYNTHESIS).
C*I*S*H* takes the advantages of subtotal hysterectomy (pelvic floor preservation, safety to surrounding pelvic structures, low morbidity) and combines them with the aim for cervical cancer prophylaxis in total hysterectomy: the cervix is not left in, yet not totally removed either.
Cancer prophylaxis is the sole purpose of removing the cervix at the time of hysterectomy. There are about 100,000,000 women in the United States, 600,000 of them have a hysterectomy per year. Most hysterectomies are not performed for life threatening conditions, but for reduction of suffering and to improve the quality of life. Do these relatively few cervicectomies really make an impact on the incidence of cervical cancer? Mass screening with modern detection methods and treatment of precancerous lesions appears to be better prophylaxis.
C*I*S*H* preserves the pelvic floor structures: prophylaxis against possible prolapses, bladder, and bowel dysfunction.
Emotional and psychological sequelae deserve our attention. The attitudes and feelings of the male partner call for serious consideration.
[prev.page]
[next page]
[contents]
[home]
P.F. Vietz, M.D.
Westminster, MD. 21157 (USA)
mailto:pvietz@qis.net
September 1997